RESEARCH NOTES: The Body Keeps the Score Part 3
Part 3 of this book, Titled "The Minds of Children" sat a bit differently for me than the previous sections. While my accident and subsequently, the art I intend to create, deals with Post Traumatic Stress as it presents itself following a single accident, this section, focusing on long term trauma experienced in early development had much fewer things for me to relate to, and in, my work.
In a lot of ways, I felt validated in this stance when, towards the end, Dr. van der Kolk explained what he and many others believe is the problem with symptom based diagnosis. Their proposal, that long term childhood trauma be relabeled as an overlapping but separate diagnosis as Developmental Trauma Disorder (DTD), has been rejected, currently, by the handbook on mental diagnosis. At the very least, the section of the book implies greatly that DTD would occur as a subset of Complex PTSD, whereby the trauma produces symptoms that develop after long exposure, in this instance, primarily the first few years of life.
Because of this, it is not too hard to see why I was not able to pull as much from this section in terms of research - it is not that it is not interesting or informative, it is only that the contents of it deal with a more or less unrelated state of mental health.
I will post my notes from this section below:

The Problem with Diagnosis
- "Insurance companies require a DSM (Diagnostic and Statistical Manual of Mental Disorders) diagnosis for reimbursement"(p.139)
- The implications here are that the chief goal of creating diagnoses for people is to justify to insurance companies to pay for treatments of delineated disease.
- What it does not do is lead to the necessary treatment for each individual.
"treatment needs to address not only the imprints of specific traumatic events but also the consequences of not having been mirrored, attuned to, and given consistent care and affection: dissociation and loss of self regulation" p. 124
Some people start using their diagnosis as their identifier and treat it like a prison sentence.
The definition of diagnosis: "a.) The act or process of identifying or determining the nature and cause of a disease or injury through evaluation of patient history, examination and review of laboratory data. b.) The opinion derived from such an evaluation" (p.140)
DMS definition of PTSD: "A person is exposed to a horrendous event that involved actual or threatened death or serious injury, or a threat to the physical integrity of self or others causing intense fear, helplessness or horror." (p.159)
- Having a PTSD diagnosis from a single event can be effectively treated (such as me)
- However, children experiencing repeated childhood trauma do not even qualify for a PTSD diagnosis and can accumulate multiple interconnected diagnoses instead that only treat symptoms like "throws tantrums" and "will not listen to me"
- The treatments, such as medication, behavior modification & exposure therapy can do more harm than good for these patients.
Tried to make a diagnosis for this type of long term trauma "Developmental Trauma Disorder"
- Consistant profile:
a. consistent pattern of dysregulation
b. problems with attention and concentration
c. difficulty geting along with themselves and others (all p.160)
- Many individuals experiencing DTD are given multiple labels of diagnosis based on symptoms, which tell what their symptoms are without treating the underlying causes of those symptoms.
DTD was not considered for the latest addition of DSM because it was said not to have filled a "missing diagnostic niche" (p.161)
The biggest issue with how the DSM defines mental illnesses has to do with how diagnosis is treated in a symptomatic way, not in a way that addresses underlying causes. As Dr. Kolk describes it in the book, "DMS medical psychiatry firmly regressed to early-nineteenth-century medical practice" (p.166) by ignoring these root causes to manage symptoms. Basically, since the diagnoses listed there cannot produce reproducible results, the DMS lacks scientific validity.
- a nice scathing report of the DMS as a tool, honestly. He implies very heavily on page 167 that the only reason they keep making more versions of it and expanding the diagnoses it carries is for the purposes of making money off of the mental health practitioners, lawyers, social workers etc who will have to purchase it to feel up to date.

Children & Caregivers
Children who suffered from trauma suffer from severe "disturbing" symptoms:
- Inconsistent clinginess
- Compulsive masturbation
- hitting & biting
- lashing out at others, objects, animals & self
Some of these children could not recognize themselves in the mirror
Trauma and inconsistent parenting had left them unable to develop a sense of self at the foundation level - from how their caregivers respond to them.
"our most intimate sense of self is created in our minute-to-minute exchanges with our caregivers" p. 111
Children choose, early on, one adult (or a few) who their natural communication starts creating attachment bonds.
- When infants and small children do not see their primary care giver giving them attention they get anxious.
- They attune with these adults and mirror their responses to experience and sensations
Being in sync with their primary adult figure:
- Being in sync emotionally = being in sync physically
Learning how to manage Arousal is done by parents first (hunger, fear, wetness ect)
When the baby feels and uncomfortable sensation, the adult manages it by feeding, comforting, drying ect, which then causes associations in the babies brain to develop between discomfort and safety, comfort and mastery (rather than continued fear)
- This leads to both agency & empathy for others situations
Neglect of self & giving up can be conditioned as well when children are neglected or abused by a caregiver.
"In order to know who we are - to have an identity - we must know (or at least feel that we know) what is and what was "real." We must observe what we see around us and label it correctly; we must also be able to trust our memories and be able to tell them apart from our imagination. Losing the ability to make these distinctions is one sign of what psychoanalyst William Niederland called "soul murder." Erasing awareness and cultivating denial are often essential to survival, but the price is that you lose track of who you are, of what you are feeling, and of what and whom you can trust. (p.136)
Attachment
The attachments children have to their primary care giver come in one of 3 types looking at how children react to temporary seperation from their mother (research of Mary Ainsworth & Mary Main)
1. Secure Attachments - children experience distress when mother leaves , and delight at their return.
- Play will soon recommence
2. Insecure: 2 distinct responses depending on how the parent behaves around the child
a. Avoidant Attachments
- Infant appears unbothered: no crying, ignores when comes back
- arousal still occurs on the interior (heart rate)
- "dealing but not feeling" p. 118
Avoidant mothers don't like touching their children
b. Anxious / Ambivalent Attachments
- draw attention to themselves constantly: crying, tantrums, clinging, screaming
- Upset when mom leaves, but not comforted by her return
- "Feeling but not dealing" p.118
Either way, consistent patterns of care, regardless of if it is Secure or Insecure, create children who can adapt to maintain the relationship.
The bulk of children with substantial mental health issues belong to none of the above groups but instead do not know how to deal with their primary care giver
3. Disorganized Attachment
- unable to figure out how to engage with caregivers.
- Caregivers are the source of terror or rage
Caregivers are both necessary for survival AND the source of fear
They freeze, unable to choose between seeking closeness or avoidance from the parent.
- Alternatively, they either trust complete strangers or no one at all
- "freight without solution" p.119
Displays itself in 2 Ways
1. Preoccupied
- Mothers are too preoccupied with own needs to respond to baby needs.
- reject their infants or believe the infant should respond to their needs
- Mothers often have history of physical abuse / Domestic violence
2. Helpless or Fearful
- Don't know how to be the adult
- Want their children to comfort them
- Mothers often have history of sexual abuse / parental loss
None of this implies one must be a perfect parent, however - you wont automatically fall into a disorganized attachment by setting boundaries or feeling the occasional impatience or anger. Kolk describes how "good enough" caregivers can repair broken connections with kids and that the "critical issue is whether they can incorporate feelings of being viscerally safe" with caregivers (p.119)

The Cycle of Trauma
Traumatized parents have a hard time connecting consistently with their children leading to disorganized attachment. In other words, the trauma of the parent comes to affect children, and children who's parents are traumatized show a predisposition to trauma themselves. Mis-attunement that occurs often can lead to chronic disconnection and therefore disorganized attachment.
Children often do not say anything to other adults about being abused because they believe that if they tell someone and break that trust with their abusive caregiver then they will be punished. They see their caregiver as the ultimate authority over them. This is not exclusive to children either.
Role Reversal
- When a baby is neglected or abused, the parent may treat the child as if the child should tune itself to fit the parents needs, leading to role reversal.
"The baby learns to become the mother's idea of what a baby is" p. 115
Non traumatized children develop an understanding of voices and faces and will adjust behavior accordingly
Traumatized children are hyper vigilant about all changes in face and voice, but respond as threats over trying to get in sync with others
- Some become meek and others put up a tough front.
Those who do not find ways to make healthy relationships or connections will connect through unhealthy means: arguments, illness, lawsuits, etc. rather than be alone
ie: Kids who get in trouble with authority just because it means someone is paying them attention.
Role reversal has shown to be more damaging through aggressive behavior and self harm in young adults than hostile behavior on the part of the caregiver.
Dissociation: n. "the feeling of being lost, overwhelmed, abandoned & disconnected from the world; seeing oneself as unloved, empty, helpless, trapped & weighed down" p(. 123)
Can occur when caregiver ignores needs & resents your existence
- Children learn to block out the looming hostility and act as if it does not matter
- still leads to heightened state of arousal
"Dissociation means simultaneously knowing & not knowing" (p. 123)
Self harm can often pair itself with dissociation, as the extreme lengths of cutting, burning or pinching oneself can be an effort to feel anything.
While occasional dissociation can occur with other trauma, Chronic dissociation cannot be accounted for by trauma alone
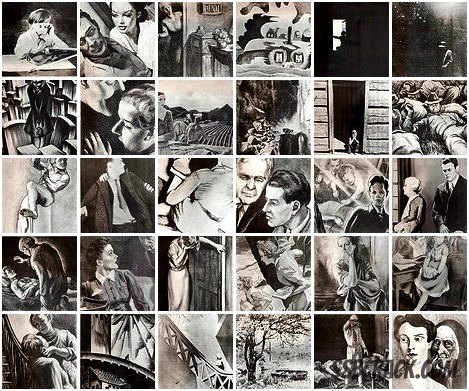
Thematic Apperception Test (TAT)
Uses neutral images on a set of cards to see how their inner reality shapes their world view
- depicts realistic but ambiguous & somewhat troubling scenes
- Subjects asked to tell stories about what is going on in the photo
- the themes of their story show the themes and situations which preoccupy them
- Control children told positive or benign stories
- Traumatized children told violent or gruesome stories
"for abused children, the whole world is filled with triggers" p.110
The question now is: Can traumatized children learn their way out of trauma brain?
*** I am curious if this is something I could use in conjunction with my game in some why. To that end, this whole process reminds me of how I view the use of Tarot Cards. While I do sometimes give myself tarot readings, I look at it from a much less spiritual perspective. Drawing the cards and reading the fortunes allows me to see what parts of the "fortune" resonates with my current situation and see what I am preoccupied by during times of indecision. I would have to do more research into this, but would Tarot cards be implemented in the game with this same kind of neutral world view?
* Might make an interesting collectable with the ability to respond to how each individual player responds to a situation. Perhaps using some kind of order vs chaos mechanic?
How to Take Trauma History
This can be difficult, as people feel shame about trauma and try to hide or underplay the trauma that was experienced.
Kolk & co came up with the Traumatic Antecedents Questionaire to gather trauma data through subtle questions that lead to conclusions about trauma - without addressing it directly
They found that the impact of abuse and the susceptibility of abuse victims to other comorbidity (BPD etc.) was dependent on when the abuse began - generally before the age of 7 is the demarcation line for the most severe long term effects.

Different Groups of Trauma: PTSD vs Complex PTSD
One study of 525 adult patients found that they fell into 3 distinct groups:
1. Longterm survivors of physical or sexual abuse
2. Recent victims of domestic violence
3. Those who recently survived a natural disaster.
The far ends of the spectrum are:
Natural Disasters --------------- Long Term Sexual/Physical Abuse
Those in natural disasters rarely experienced self loathing, navigating relationships, memory gaps, self destructive behaviors and other medical problems.
** I am intrigued at the suggestion that this is a spectrum rather than three concrete groups overall. While I feel I definitely lean more towards the less destructive side from my experience (Natural Disasters) I have experienced some of these more serious symptoms. A spectrum feels as though it counts more towards the individual.
Kolk and others tried to create a new diagnosis for those who experienced interpersonal trauma: "Disorders of Extreme Stress, Not Otherwise Specified" (DESNOS) aka Complex PTSD, however, the DSM did not put it in their final book. They decided it was not dissimilar enough from the current definition of PTSD to warrant its own subset.
- **I do find it interesting, however, that in spite of this set back, I have often heard Complex PTSD used in the vernacular anyway.
"The consequences of caretaker abuse and neglect are vastly more common and complex than the impact of hurricanes or motor vehicle accidents" (p.145)
- **I highly agree with this statement. Part of the reason I decided to use a person vs environment narrative for my PTSD game is not only because it matches my experience but because it seemed plausible to do for a thesis project given the resources I currently have. That is not to say I would not be interested in working on something more complex in the future.
Complex PTSD
- Childhood trauma is far more common than anticipated
- "Insidents of abuse are never stand-alone events. And for each additional adverse experience reported, the toll in later damage increases" (p.147)
The isolation and lack of protection stemming from childhood trauma can lead the traumatized individual to believe that death is the only escape available to them. This accounts for the higher suicide rates in trauma victims - both children, adults and veterans.
Problems as Solutions: Some public health problems actually act as personal solutions for trauma
- for instance, obesity can give comfort to a rape victim because they feel as though they will be overlooked and therefore safer.
- long term health risks can give short term benefits that are hard to give up. The individual is instead weighing the costs and benefits.
The public health studies concluded about this type of mental disorder have not lead to widespread changes, unlike their biological counterparts such as heart disease. There are no sweeping changes here.
Nature vs Nurture
Thus far, there has been no answers in genetics as for factors that predispose people to develop PTSD.
However, while genes cannot be altered at the fundamental level, Methylation patterns (clusters of carbon and hydrogen atoms on the outside of a gene that turn on and off biological messeges) CAN be passed off to offspring and possibly predispose people to the development of PTSD.
However, major changes to this biology rely on more than genetics but also focus on how the social world reacts to the human brain. *An externalist perspective, not simply an internalist one.
Experiment involving Rhesus Monkeys showed that two types of monkey personalities ran into relationship trouble:
1. Uptight monkeys - fearful, withdrawn and depressed
2. Aggressive monkeys - make so much trouble they are shunned, beaten or killed.
Biologicially both types have abnormality caused in their first few weeks of life
Social environmental factors contribute as well. Stable social groups lead to diligent mother monkeys. Lack of a social network (such as the uptight monkeys) lead to a high risk of neglect or abuse of their children. Monkeys taken away from their mothers and raised together form intense social attachments to each other
- Peer raised monkeys will always over react to minor stresses, much more than the others, even monkeys brought up by aggressive mothers.
Other details from the section:
It is not important to know every detail of someone's trauma to help them.
Trauma causes auto immune responses and makes it over sensitive to threats. this can cause auto immune disorders where the cells will attack the body.
Dr. Kolk states how he does not tell patients how they should be feeling, even if their feelings are objectively the wrong way to feel (ie: blaming themselves for their abuse)
- this is due to a patient who informed him that telling them that they shouldn't feel the way they are makes them feel isolated and stupid and "confirms the feeling that nobody in the whole world will ever understand what it feels like to be [them]" p. 130
Just to reiterate, trauma is not a chronological narrative but fragments of experiences, images, sounds, and sensations with no feelings besides panic and fear.
Finally, I also deeply appreciate Dr. Kolk's scathing opinion of the United States current abysmal state of mental health practices, particularly in terms of preventative measures to keep people out of the prison pipeline system. Good for you, man!

Comments
Post a Comment